
People can have different kinds of problems with their breasts. The important thing to know is that in most but not all cases, breast-related problems are not caused by breast cancer. Even so, if you develop any problem with your breasts, see a doctor or nurse to have it checked out.
Some common breast problems include:
Breast Lump:
You or your healthcare provider may find a breast lump by looking at or feeling your breast. It is difficult to determine by examination alone if a lump is caused by breast cancer. Although most breast lumps in women age 20 to 50 are not cancerous, all new breast lumps should be evaluated by a healthcare provider to determine if further testing is needed.
- Evaluation — After a breast examination, the best test for evaluating a breast lump depends, in part, upon your age.
- Women under age 30 — If you are under 30 years and you find a lump before your menstrual period, you may be advised to have a repeat breast examination after your period has ended. In this age group, breast lumps are often caused by hormonal changes and will resolve after your menstrual cycle.
If the lump does not go away when your period is over, you will likely need further testing with a breast ultrasound or needle aspiration biopsy to determine whether the lump is fluid filled or solid. Mammograms are not usually performed in women under 30 years old, although a mammogram may be needed if the ultrasound does not provide enough information. - Women age 30 and older — Women who are age 30 or older who find a new breast lump will need a diagnostic mammogram, and usually an ultrasound, as well. During a diagnostic mammogram, a mammography technician works with a radiologist to study the area that feels or appears abnormal. Often, a mammogram of the other breast is done for comparison. If the lump appears suspicious on the mammogram and/or the ultrasound, a breast biopsy is usually recommended.
- Ultrasound and needle aspiration — Ultrasound of the breast may be recommended to determine whether a lump is fluid filled or solid. Needle aspiration (using a needle and syringe to withdraw fluid) is another option.
– Fluid-filled cysts are not usually caused by cancer and only require treatment if they cause discomfort. Treatment for a fluid-filled cyst, if necessary, usually includes draining the fluid with a needle.
– Women with a solid or “complex” (fluid and solid) breast nodule are usually advised to have a biopsy.
- Breast biopsy — A breast biopsy is often recommended to further evaluate a new breast lump. A breast ultrasound, mammogram, or needle aspiration may be recommended before a biopsy.
If your healthcare provider can feel the lump, s/he can often biopsy the area with a needle right in the office. This may involve removing some cells (fine needle aspiration) or a small sample of tissue (core needle biopsy).
If the abnormality cannot be easily felt but is visible on the ultrasound, a needle biopsy can be done under ultrasound guidance. This involves placing a needle in the abnormal area and removing a sample of tissue, which is later examined with a microscope.
If the abnormality can be seen only on the mammogram, there are two ways to biopsy the area:
– A needle biopsy may be done in radiology with local anesthesia using mammographic guidance (called stereotactic biopsy).
– Occasionally, biopsies must be done surgically instead. In this case, the radiologist will work with the surgeon to mark the abnormal area with a thin wire, radioactive or magnetic seed, or another method prior to surgery. After the radiologist places the seed or wire, the surgeon can use it to guide removal of the proper area. Surgical biopsy is usually recommended only if the biopsy cannot be obtained with less invasive methods.
Abnormal mammogram:
Having an abnormal screening (initial) mammogram can cause concern. Fortunately, most women with abnormal mammograms do not have breast cancer. An abnormal mammogram may be due to a mass, a collection of calcium deposits (called calcifications), or other factors. Sometimes, normal breast structures can overlap in a way that can look abnormal even if nothing is really there.
If you have an abnormal screening mammogram, the next step depends on the type of abnormality found.
- If the abnormality is likely benign (not cancerous), you may be advised to have a follow-up mammogram in six months.
- If the mammogram shows an area that is abnormal, the next step is to have additional imaging, such as a diagnostic mammogram. During a diagnostic mammogram, a mammography technician works with a radiologist to study the area that feels or appears abnormal. Different angles can be used, and the picture can be magnified and/or targeted to a particular area of interest. The radiologist can usually review the mammogram immediately and discuss the results with you. In some cases, an ultrasound may be performed to better define the abnormality.
In many cases, the diagnostic mammogram shows that the abnormality is benign (not cancerous), and no further testing is needed. However, if the diagnostic mammogram is indeterminate or suspicious for cancer, a breast biopsy is recommended.
- Occasionally, other types of breast imaging, such as magnetic resonance imaging (MRI), may be required to further evaluate the abnormality found on mammogram.
Breast Pain or tenderness:The most common type of breast pain is caused by the hormones that control the menstrual period. These hormonal changes can cause pain in both breasts several days before the menstrual period begins. Because the pain can come and go with the menstrual cycle, it is called “cyclical” breast pain. Cyclical breast pain is not usually caused by breast cancer or other serious breast problems. Breast pain in the perimenopausal years may also be related to hormonal changes.
Less commonly, a woman can have breast pain that does not come and go with the menstrual cycle (also called noncyclical breast pain). This type of pain is not related to the menstrual cycle and might occur in only one breast or one area of the breast. Noncyclical breast pain is usually caused by a problem outside the breast, such as muscle or connective tissue strain, skin injury, spinal conditions, or problems in another organ system (eg, heart burn, chest pain). Noncyclical breast pain is caused by breast cancer in only a very small percentage of women.
If you are worried about breast pain, speak to your healthcare provider to determine if you need further testing. If testing shows no signs of a serious problem, you can try one or more of the following treatments:
- Pain relief medicines, such as acetaminophen (Tylenol and others) or ibuprofen (Advil, Motrin, and others). Women with very severe breast pain are sometimes treated with a prescription medicine.
- Decrease the dose or stop taking medicines that contain estrogen (after a discussion with your healthcare provider).
- Wear a well-fitted support or sports bra.
- Consider making changes to your diet. Elimination of caffeine and a low fat, high complex carbohydrate diet is helpful for some women. Dietary supplements such as vitamin E and evening primrose oil have also been suggested for breast pain; however, there is no proof that these are effective.
Nipple Discharge: Having a milky-colored discharge (also called galactorrhea) from both nipples is common, especially during the first year or two after giving birth. Nipple discharge from both breasts can also occur in women with an underactive thyroid (hypothyroidism), as a side effect of certain medications, or because of a growth in the pituitary (a part of the brain), causing an increase in a hormone called prolactin
As with other ducts in the body, breast ducts make and carry secretions. Many women can express (squeeze out) a small amount of yellowish, greenish, or brownish discharge. This is often called “physiologic” discharge and is not a cause for concern. Physiologic discharge is not bloody.
Spontaneous nipple discharge (discharge that occurs without squeezing) or nipple discharge that is clear (not yellow or straw-colored) or bloody may be caused by an abnormal growth within the breast or, less commonly, by breast cancer.
Any woman with nipple discharge should be evaluated by a healthcare provider. A mammogram, breast ultrasound, breast magnetic resonance imaging (MRI) scan, and/or exam of the breast ducts (ductogram, also called galactogram) may be recommended in some cases.
Inverted Nipples: Many women are born with nipples that naturally invert (pull in) at times and evert (poke out) at other times (sometimes called “bifid,” “cleft,” or “slit-like” nipples). Other women find that this happens after breast feeding. Nipple inversion of this type is not cause for concern.
If your nipples have always been everted, however, and begin to invert for no obvious reason, this should be evaluated by your healthcare provider. Most causes of nipple inversion are not a cause for concern, but occasionally this is the first sign of a breast cancer. New nipple inversion is usually evaluated with a breast examination and mammogram as a first step.
Breast skin Changes: Skin problems can develop on or near the breast, some of which cause itching, scaling or crusting, dimpling, swelling, redness, or changes in skin color. While most of these changes are not caused by a serious breast problem, it is important to be evaluated if a skin problem on your breast does not resolve within a few days.
More serious causes of skin changes on the breast can include less common forms of breast cancer, such as Paget disease or inflammatory breast cancer. Other, more common skin problems, such as rashes, moles, cysts, or skin infections, can occur on the skin of the breast, as well.
The evaluation of breast skin changes usually includes a breast examination and may include a mammogram. A skin biopsy may be needed to confirm the diagnosis.
These problems can happen at any age. If you develop any of these problems, see your doctor or nurse. Breast problems are not usually an emergency, but you should get checked out as soon as possible. If there is something serious going on, it’s important to find out quickly. Your doctor or nurse might be able to tell what’s happening just by doing an exam. If not, they can order some tests, or send you to a specialist.
- Breast ultrasound – This is an imaging test that uses sound waves to create pictures of the inside of your breast. Among other things, it can show if a lump is solid or filled with fluid.
- Breast biopsy – During a biopsy, a doctor takes 1 or more tiny samples of suspicious breast tissue using a needle. The samples then go to the lab to be checked for cancer or other problems.
- Mammogram – Mammograms are special X-rays of the breast. They can help doctors find breast cancer.
The goal of breast cancer screening is to find cancer early, before it has a chance to grow, spread, or cause problems. Studies show that being screened for breast cancer lowers your chance of dying of the disease.
Starting at the age of 40, it’s important to talk to your doctor or nurse about the benefits and drawbacks of screening and decide, with your doctor or nurse’s help, whether to get screening and when.
Some people who are at high risk of breast cancer might need to begin screening before age 40. Talk to your doctor or nurse to see if you should start screening earlier. For example, you might do this if you are under 40 but have a relative who got breast cancer at a young age, or if you have certain genes that increase your risk of breast cancer (such as “BRCA” genes).
Regular screening with mammograms generally continues through age 74 years. Some people choose to continue getting regular mammograms after this if they are healthy and expected to live for at least 10 more years.
Some people have had temporary swelling of lymph nodes in the armpit area after getting certain COVID-19 vaccines. In some cases, this can make it harder for doctors to interpret your mammogram. For this reason, experts recommend trying to schedule your mammogram either before you get the COVID-19 vaccine, or at least 4 to 6 weeks after your last dose.
If you’re not sure when to schedule your mammogram, talk to your doctor or nurse. They can help you make this decision based on your situation. While breast cancer screening is important, it is also very important to get the COVID-19 vaccine when you are able.
- False positives – Mammograms sometimes give “false positive” results. This means they suggest that you might have cancer when you actually do not. This can lead to unneeded worry and to more tests – including a biopsy in some cases, which can be painful. False positive results are more likely to happen in people younger than 50 than they are in older people.
- Finding cancer that would not have needed treatment – Sometimes, mammograms find cancer that would never have affected your health. This can be a problem because treating these cancers does not have any benefit, and can cause harm. For example, you could get surgery, radiation treatment, or chemotherapy to treat a cancer that never would have caused problems if it hadn’t been found. There is no way to know which cancers found by screening will lead to problems, and which won’t.
- Radiation exposure – Like all X-rays, mammograms expose you to some radiation. But studies show that the number of lives saved by finding cancer early greatly outweighs the very small risks that come from this radiation exposure.
There are different types of machines that are used for mammograms. They include film mammography, digital mammography, and something called “digital breast tomosynthesis” or “DBT.” DBT creates images of the breast from different perspectives. It is sometimes called “3-D mammography.”
Getting a mammogram can be uncomfortable, but it lasts only a few seconds. If your breasts are sensitive before or during your period, you might want to avoid scheduling your mammogram during that time, if possible. Also, do not use underarm deodorant or powder on the day of your appointment.
If the doctor thinks your abnormal result is probably not due to cancer, they might suggest that you have another mammogram in 6 months. In other cases, the doctor will send you for more tests. This could be because they need to get a better view of part of your breast, or because they think the abnormal result might be due to cancer. Other tests could include a more detailed mammogram, which involves taking more X-rays to get a better view, or an ultrasound of the breast to check something seen on mammogram. An ultrasound or MRI might also be suggested if your mammogram shows very dense breasts that can make a mammogram harder to read.
If these tests show any suspicious findings, your doctor or nurse will probably order a biopsy. During a biopsy, a doctor takes a sample of breast tissue and sends it to the lab to be checked for cancer. Biopsies are usually done by taking some tissue from the breast with a needle during a mammogram or ultrasound. But in some cases biopsies involve a small surgery.
Some people want to do exams on their own breasts. No study has shown that breast self-exams lower the risk of dying from breast cancer, and most experts do not encourage self-exams. Some experts encourage something called “breast self-awareness.” This involves learning about your personal risk of breast cancer, what your breasts look and feel like normally, and what to do if you do notice a change in your breast. If you notice any changes in your breasts, talk to your doctor or nurse.
- The size and location of the abnormal area
- What the abnormal area looks like on your ultrasound, mammogram, or MRI
The 3 main types of biopsies are:
- Fine needle biopsy – For this type of biopsy, the doctor uses a very small needle to remove a small amount of tissue or fluid from the abnormal area.
- Core needle biopsy – For this type of biopsy, the doctor uses a larger needle with a special tip. Often the doctor will also use special imaging equipment to find the abnormal area to take the biopsy. There are different ways to do this:
Ultrasound-guided biopsy – If you have this type of biopsy, you will lie on your back or side and the doctor will hold the ultrasound device against your breast to guide the needle.
Stereotactic biopsy – For this type of biopsy, you will most likely lie face down on a table. The table has an opening for your breast, which is pressed between 2 metal plates, just like it is during a mammogram. During this type of biopsy, the doctor takes an X-ray to decide where to insert the needle.
Tomosynthesis-guided biopsy – This also involves using X-rays to help guide the needle, as with a stereotactic biopsy. It requires a special machine that takes multiple X-rays to create a three-dimensional image of your breast. This is also called a “3-D mammogram.”
MRI-guided biopsy – If you have this type of biopsy, the doctor will use an MRI scan to decide where to take the biopsy. MRI uses a special type of magnet to create pictures of the breast.
After a core needle biopsy, your doctor will place a tiny piece of metal, called a clip, in your breast. The clip can be seen on an ultrasound or X-ray, so that in the future, doctors can see where the biopsy was taken. You cannot feel the clip and it will not cause problems during future imaging tests, including airport screening tests. - Surgical biopsy – A surgical biopsy is done in the operating room under anesthesia. The surgeon will make a small cut (incision) in your breast and take out the abnormal tissue. Afterwards, they will take a special X-ray to make sure the abnormal area has been completely removed.
You will likely get the results of your biopsy in about a week. Your doctor will talk to you about what the results mean and what will happen next. If the results are not clear, your doctor will schedule another biopsy or procedure to get more information.
If you feel a lump in your breast, see your doctor or nurse right away. Breast lumps can be caused by conditions that are not cancer. But it is a good idea to have any lumps checked out.
Most people with breast cancer have one or more of the following treatments:
- Surgery – Breast cancer is usually treated with surgery to remove the cancer. Many people with breast cancer can choose between 2 types of surgery:
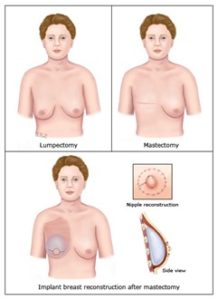
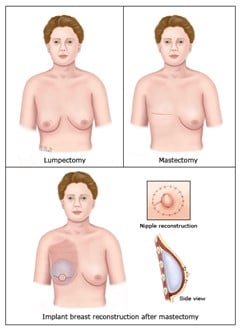
Mastectomy is surgery to remove the whole breast. (If you choose this option, you might have to decide whether to have surgery to reconstruct your breast and when.)
Breast-conserving surgery (also called “lumpectomy”) is surgery to remove the cancer and a section of healthy tissue around it. People who choose this option keep their breast. But they usually must have radiation therapy after surgery. - Radiation therapy – Radiation kills cancer cells.
- Chemotherapy – Chemotherapy is the medical term for medicines that kill cancer cells or stop them from growing. Some people take these medicines before surgery to shrink the cancer and make it easier to remove. Some take these medicines after surgery to keep cancer from growing, spreading, or coming back.
- Hormone therapy – Some forms of breast cancer grow in response to hormones. Your doctor might give you treatments to block hormones or to prevent your body from making certain kinds of hormones.
- Targeted therapy – Some medicines work only on cancers that have certain characteristics. Your doctor might test you to see if you have a kind of cancer that would respond to this kind of therapy.
- Immunotherapy – This is the term doctors use for medicines that work with the body’s infection-fighting system to stop cancer growth. Immunotherapy might be used with chemotherapy to treat certain types of advanced breast cancers.
Getting treated for breast cancer involves making many choices. Besides choosing which surgery to have, you might have to choose which medicines to take and when.
Always let your doctors and nurses know how you feel about a treatment. Any time you are offered a treatment, ask:
- What are the benefits of this treatment? Is it likely to help me live longer? Will it reduce or prevent symptoms?
- What are the downsides to this treatment?
- Are there alternatives to this treatment?
- What happens if I do not have this treatment?
A sentinel lymph node biopsy for breast cancer is an operation to check if your breast cancer has spread to your lymph nodes.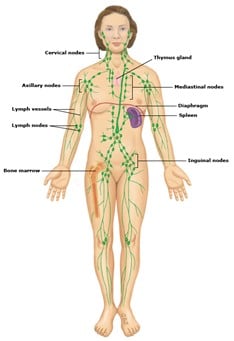
ImageLymph nodes are bean-shaped organs found all over the body, including the armpits, neck, and groin. They are part of a network of vessels called the called the “lymphatic system,” which carries a clear fluid called “lymph”. When breast cancer cells spread, they usually travel first through the lymph to 1 or more lymph nodes in the armpits. These lymph nodes are called “sentinel lymph nodes.”
During a sentinel lymph node biopsy a surgeon finds, takes out, and checks the sentinel lymph node (or nodes) for cancer cells. Knowing whether cancer is in the sentinel lymph nodes helps your doctor choose the right treatment for your breast cancer.
A sentinel lymph node biopsy is also called an “SLNB.”
The operation is usually done under general anesthesia. This means you will get medicines through a small tube into a vein (called an “IV”) or gases that you breathe through a mask to make you unconscious.
Doctors use 2 different techniques to find the sentinel node:
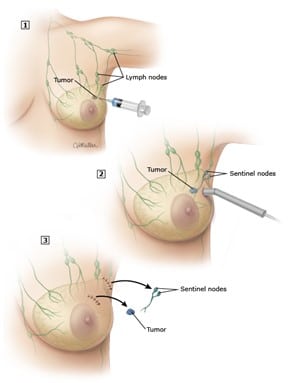
- Blue dye – For this technique, the doctor injects blue dye into your breast near the cancer after you are unconscious in the operating room. The dye travels through the lymph and turns the sentinel node blue.
- A radioactive substance – For this technique, the doctor injects a radioactive substance into your breast near the cancer and the colored area around your nipple, before you go to the operating room. Then, after you are unconscious, the doctor uses a special device that finds radioactive substances to locate the sentinel lymph node.
Most surgeons use both of these techniques, but some use just 1. After finding the sentinel node, the surgeon makes a small cut to take it out, then sends it to a lab. A different doctor then checks the node for cancer cells. Often, more than 1 sentinel node is found and taken out.
Most people do not have cancer in their sentinel lymph nodes. But if they do, the surgeon might take out other lymph nodes in the armpit to check them as well. If this happens, it is usually during a separate operation.
After an SLNB, you might have pain, bruising, bleeding, or get an infection. Your doctor will prescribe pain relievers or other medicines to treat any symptoms.
If your doctor used blue dye, part of your breast will be blue until all of the dye disappears from your body. Your urine will also turn green for 1 day.
In rare cases, people are allergic to the dye used for SLNB. Your doctor will tell you about this risk and answer any questions you have before the operation. The allergic reaction happens in the operating room and is treated right away with medicines given through an IV.
If your doctor used a radioactive substance, the amount of radioactivity is very low and not harmful. It leaves your body quickly through your urine. You are not “radioactive” or dangerous to other people near you.
Your doctor will let you know about the result of the biopsy. They will also tell you if additional lymph nodes need to be removed from your armpit.
- “Local treatment” – This is treatment directly to the breast with surgery or radiation.
- “Systemic treatment” – This is the name for medicines that treat the whole body. Chemotherapy is one example. There are other medicines that can be used, too. They destroy cancer cells or stop them from growing. They also lower the chances that the cancer will return anywhere in your body.
- Mastectomy – This is surgery to remove the whole breast. Most people who have a mastectomy can also have surgery to reconstruct the breast that is removed.
- Breast-conserving therapy (also called “lumpectomy”) – This is surgery to remove the cancer and a section of healthy tissue around it (called a “margin”). People who choose this option keep their breast. But they usually must have radiation therapy after surgery to kill any cancer cells that might still be in the breast area.
No. Studies show that people who choose lumpectomy live just as long as those who choose mastectomy.
| Mastectomy | Lumpectomy |
How will I look? | If you decide not to have your breast reconstructed, you will have a scar where your breast used to be. If you do have your breast reconstructed, you will have a new breast made of an implant or out of skin, muscle, and fat taken from other parts of your body. Reconstructed breasts do not have as much sensation as breasts that have had a lumpectomy. | Your breast will have a scar and might have a dent or dimple where the tissue was removed. The treated breast might be a little smaller than the other breast. Still, it will feel more like a real breast than a reconstructed breast and have more sensation. |
What will my recovery from surgery be like? | You will stay in the hospital for 1 to 2 days (or a little longer if you have reconstruction done, too). You will go home with drains that must be emptied twice a day and that stay in for about 2 weeks. Your recovery will take 4 to 6 weeks. During that time, you will need to rest and avoid sports, swimming, and heavy lifting. You might need physical therapy. | You will go home from the hospital the same day as your surgery, and your recovery will take 1 to 2 weeks. During that time, you will need to rest and avoid sports, swimming, and heavy lifting. You might need physical therapy. |
What are the risks or side effects of this surgery? | Mastectomy is usually safe, but it can sometimes lead to bleeding, infection, or fluid build-up. Plus, the surgery can sometimes damage the skin on the chest. (This is more common in people who smoke.) | Lumpectomy is usually safe, but it can sometimes lead to bleeding, infection, or fluid build-up where the cancer was removed. |
Will I need more than 1 surgery? | Possibly, if you decide to have your breast reconstructed later. | Possibly, if the cancer comes up to the margins and the surgeon has to take more tissue. |
Will I need radiation therapy? | Probably not. But some people who have mastectomy do need radiation. | Yes. After lumpectomy, most people must have radiation therapy 5 days a week for 3 to 6 weeks. |
What are the chances that cancer will come back in the same area? | Cancer can still recur after mastectomy because all the breast tissue cannot be totally removed. About 5 out of 100 people who have a mastectomy will have cancer come back on the chest wall after mastectomy. | Fewer than 10 out of 100 people who have a lumpectomy will have cancer recur. |
- Have more than 1 tumor in different areas of the same breast, which cannot be removed with a single cut
- Have cancer that has spread throughout the breast tissue, and the surgeon can’t get all the cancer out with a margin of normal tissue around it
- Cannot have radiation therapy, for example, because you are pregnant or have certain skin conditions
- Already had radiation to that area of your breast. (More radiation to the same area can cause too much damage.)
Coosing between mastectomy and lumpectomy
- The way you will look – Is it important to you to keep your own breast? How would you feel if your chest was flat or you had to wear a plastic breast in your bra? Ask to see pictures of people who have had the different kinds of surgery. Remember, if you choose mastectomy, can choose to have your breast reconstructed if you want. If you have small breasts and a large tumor, a lumpectomy might make your breast look quite different. In this case, mastectomy with reconstruction might be a better option. Some people do not mind having a flat chest after mastectomy, and choose not to have reconstruction.
- The risk that the cancer will come back – People who choose lumpectomy live just as long as those who choose mastectomy. They also have about the same chances of cancer returning in the breast. Most people whose cancer comes back after lumpectomy go on to have a mastectomy.
- The time involved and the side effects of radiation – After lumpectomy, most people must have radiation therapy. This usually involves getting treatments 5 days a week for 3 to 6 weeks, depending on the person’s age and other factors, although shorter treatments may be appropriate in some cases.
This type of radiation will not make your hair fall out, but it might make you tired. It will tan and possibly even burn the skin on your chest. This burn is like a sunburn and goes away fairly quickly. Toward the end of treatment, radiation can make you feel a little tired, but this is not very common and usually doesn’t last long. - Recovery from surgery
If you have a lumpectomy, you can go home from the hospital the same day as your surgery. For a week or 2 after surgery, you will need to rest and avoid sports, swimming, and heavy lifting.
If you have a mastectomy, you will stay in the hospital for 1 to 2 days after surgery. If you also have breast reconstruction, you might stay a day or 2 longer. You will go home with drains that must be emptied twice a day. After about 2 weeks, the surgeon will take the drains out in the office. If more fluid or blood builds up after the drains come out, the doctor will drain it with a needle in the office. During the draining process and for a few weeks more, you will need to rest and avoid sports, swimming, or heavy lifting. Even after you recover, you will not have normal feeling in your chest after a mastectomy. You can choose to have your breast reconstructed right away or later, or not at all.
No matter which surgery you have, you will probably need to have biopsies of your lymph nodes. This part of the surgery usually does not cause problems and is often done at the time of your breast surgery. But in some cases it can cause arm swelling, pain, or stiffness; shoulder pain or stiffness; or a nerve injury. If any of these happen to you, you might need to do special exercises or work with a physical therapist (exercise expert) to get back to normal.
People who have early-stage cancer or are having a mastectomy to prevent cancer can have the reconstruction at the same time as their mastectomy. This is called “immediate reconstruction.”
People with a later-stage or large cancer sometimes need to have radiation after mastectomy. (Radiation is a treatment that kills cancer cells or stops them from growing.) Reconstruction might be delayed until the radiation treatment is finished. This is called “delayed reconstruction.” The delay is needed because radiation could damage the reconstructed breast. There is also concern that an implant could keep radiation from reaching the right areas.
- How big your breasts are to begin with.
- If you are overweight and whether it affects your health – Your options will also depend on how much extra body fat you have and where it is.
- Whether you have other health problems – Some types of reconstruction are not recommended for people with diabetes, heart or lung disease, or other problems.
- Whether you have had surgery before – Scar tissue from surgery might affect your options, such as where donor tissue might be able to be taken from.
- Whether radiation therapy is planned – Some types of breast reconstruction are more likely to have problems related to radiation therapy.
- Your personal preferences – Some people prefer a shorter surgery and recovery time and choose implants for this reason. Some people do not wish to have man-made materials in their body and choose flaps.
A breast implant is basically a breast-shaped container that is filled with salt-water (called “saline”) or something that feels like Jell-O (called “silicone”). The implant can be inserted partly or completely under a layer of muscle in the chest.
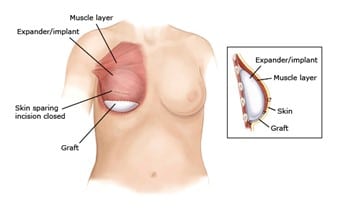
Getting an implant usually involves 2 steps. First, the surgeon inserts a device called an “expander.” Often another piece of material (called “ADM”) is added to support the expander, and later the implant. The expander stretches the skin and muscle in the chest. The surgeon gradually adds more and more fluid to the expander until the skin and muscle are stretched enough for the size of the implant being used. Then, the surgeon does another surgery to replace the expander with the implant. Implants are best for people with smaller breasts that don’t droop.
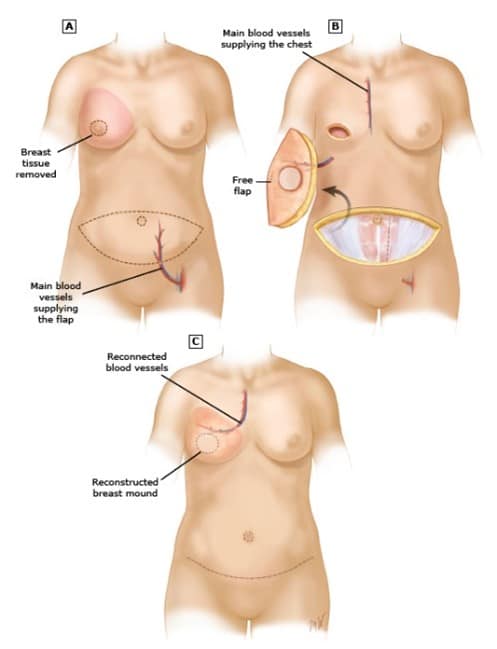
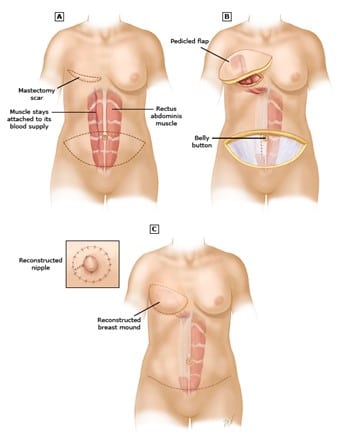
A flap reconstruction uses tissue from another part of the body to create a new breast. That tissue might be rotated in place keeping its own blood supply (called a “pedicled” flap) or disconnected and then reattached to a new blood supply (called a “free” flap). How complicated the procedure is, and the risks involved, depend on the type of tissue used.
If you choose a flap, your options might include:
- Perforator flaps – A perforator flap is the most common type of flap used for breast reconstruction. It is usually taken from the belly. One type is called a “DIEP flap”. The flap is made up of skin and fat, but not muscle. After surgery, the belly looks flatter, like it does after a “tummy tuck.” Since there is no muscle removed, the belly is not weakened after this kind of flap.
For people who do not have enough belly fat, there might be other perforator flap options.
- TRAM flaps – A TRAM flap is also taken from the belly, but is made up of skin, fat, and muscle.Because the muscle is taken, the belly is weaker after surgery. There might also be a noticeable bulge where the muscle was removed, especially if both breasts are reconstructed with this type of flap.
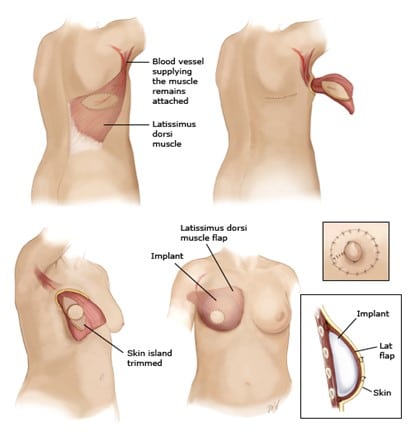
- LD flap – A latissimus dorsi (LD) flap is taken from the back and is made up of skin, fat, and muscle. People who have this kind of flap have a scar on their back, just beneath the level of the bra line. They often also get an implant, because there is not enough fat on the back to make a new breast. An LD flap is more often used when other options are not available, or if a past reconstruction has not worked out.
If you want it to be, yes. This is usually done a few months after the breast reconstruction is done. To make a new nipple, the surgeon can rearrange the tissue that is already there or use tissue from another part of the body. Surgeons can also tattoo the new nipple and area around the nipple (called the areola) to match the color of your other nipple and make it look three-dimensional.
As much as possible, yes. But the new breast will never be exactly like the breast you had before or exactly like your other breast. Plus, you won’t have normal feeling (sensation) in the new breast. If you don’t like the difference between them, your surgeon might be able to make changes to the reconstructed breast, or operate on your other breast to make them look more similar.
Maybe. Only some of the reconstruction types will be appropriate for you. But if you think you would rather have 1 type of reconstruction over another, ask your surgeon if that approach would work for you. They can tell you if your choice makes sense, and if not, why not.
Most people do not have serious problems after breast reconstruction. But there are some problems that can happen, either right after the surgery or later on:
- If you had either type of reconstruction (implant or flap) – Problems can include infection, blood or fluid coming from the area where you had surgery, or pain that does not go away.
- If you had an implant– The most common problem is called “capsular contracture.” This is when scar tissue around the implant becomes hard and tight. This can cause the breast to feel firm or sore, or change shape. Other possible problems include the implant deflating, bursting, or moving out of place.
In very rare cases, people with an implant can get a certain type of lymphoma years later. Lymphoma is a cancer of the lymphatic system, which is part of the body’s immune (infection-fighting) system. If you have an implant, it’s important to see your doctor regularly afterwards. This way they can check for, and treat, any problems. - If you had a flap reconstruction– In some cases, the flap does not get enough blood. This can happen right after surgery, or sometimes later, and if it does, some or all of the flap might need to be removed. In this case, your surgeon will need to do more surgery to fix the reconstruction, or do another type or reconstruction. Some people can develop a bulge or hernia where the flap tissue was removed to make the flap.
Call your doctor or nurse if you think you have any of these problems. Some of them need treatment right away.